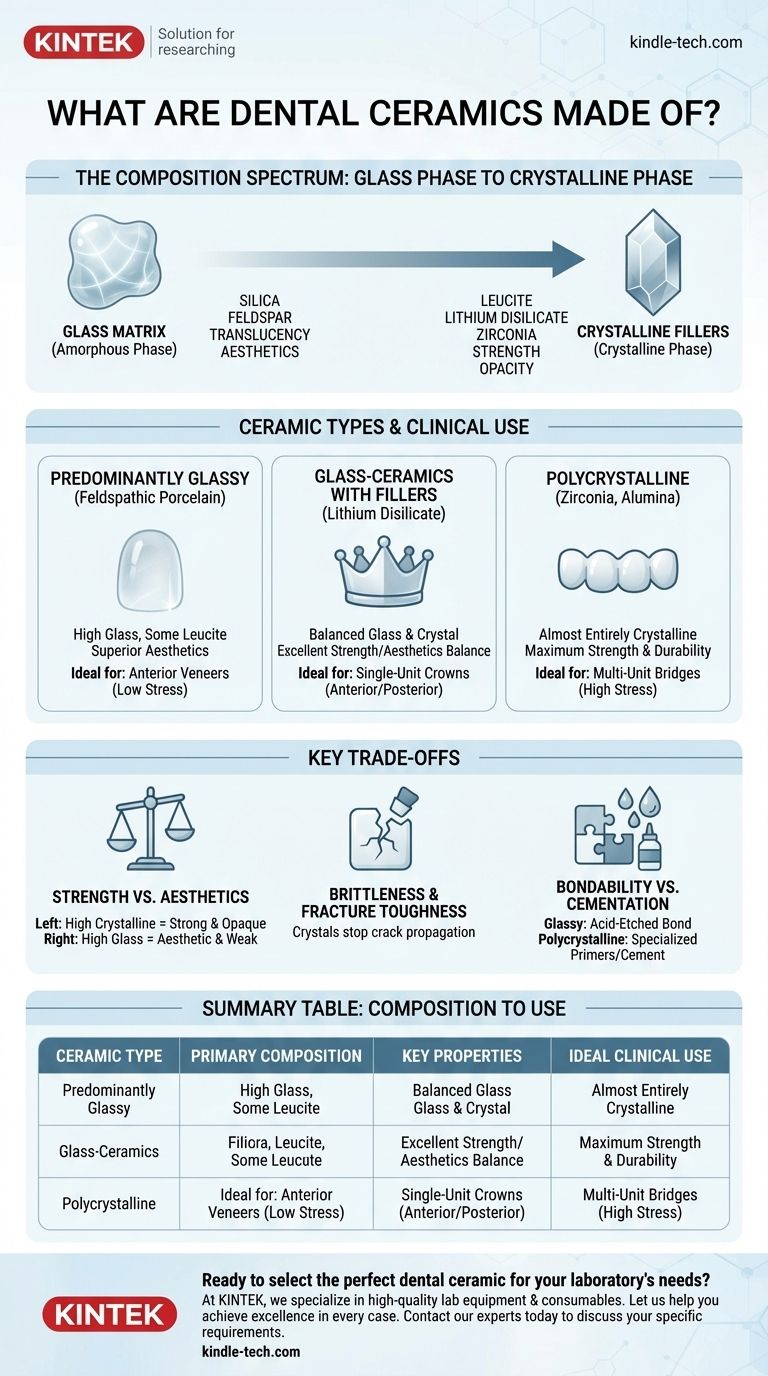
At their core, dental ceramics are inorganic, non-metallic materials composed of a carefully balanced mixture of a glass phase and a crystalline phase. They are primarily built from compounds of oxygen combined with elements like silicon, potassium, aluminum, or zirconium. This precise blend of components is what gives them their unique combination of aesthetic beauty and functional strength for use in everything from crowns and bridges to veneers.
The key to understanding dental ceramics is recognizing they exist on a spectrum. At one end is glass, which provides translucency and aesthetics. At the other end are high-strength crystals, which provide durability. The composition of any given ceramic is a deliberate choice to optimize its position on this spectrum for a specific clinical need.

The Fundamental Building Blocks
Every modern dental ceramic is designed by combining two primary structural components: a glass matrix and crystalline fillers. The ratio between these two dictates the material's final properties.
The Glassy Matrix (Amorphous Phase)
The glass phase is an amorphous (non-crystalline) structure, primarily based on silica (silicon dioxide). This forms a 3D network that gives the ceramic its translucency and enamel-like appearance.
Feldspar, a naturally occurring mineral containing potassium and aluminum silicates, is a classic source for this glassy matrix. It is the primary component in traditional porcelain.
The Crystalline Fillers (Crystalline Phase)
Dispersed within the glass matrix are crystalline structures that act as a reinforcing framework. These fillers are the source of the ceramic's strength, fracture toughness, and opacity.
Common crystalline fillers include:
- Leucite: A potassium-aluminum-silicate crystal that strengthens feldspathic porcelains.
- Lithium Disilicate: A crystal known for its exceptional combination of high strength and excellent optical properties.
- Alumina (Aluminum Oxide): An extremely hard and strong crystal used to reinforce ceramics or as a core material.
- Zirconia (Zirconium Dioxide): The strongest ceramic crystal used in dentistry, providing unparalleled fracture resistance.
How Composition Defines Ceramic Type and Use
Dental ceramics are classified based on the proportion of their glass and crystalline phases. This composition directly maps to their ideal clinical applications.
Predominantly Glassy Ceramics
These materials, often called feldspathic porcelains, are composed mostly of a glass matrix with some leucite crystals for reinforcement.
Their high glass content gives them superior aesthetics and translucency, making them ideal for cosmetic applications like anterior veneers where chewing forces are low.
Glass-Ceramics with Fillers
This category represents a significant step up in strength by incorporating a higher percentage of crystalline fillers. Lithium disilicate (e.g., IPS e.max) is the prime example.
These materials offer an excellent balance of strength and aesthetics, making them the workhorse material for single-unit restorations like anterior and posterior crowns.
Polycrystalline Ceramics
These materials consist almost entirely of crystalline structures with no intervening glass matrix. Zirconia and, less commonly today, alumina fall into this category.
By eliminating the weaker glass phase, these ceramics achieve the highest possible strength. This makes them the definitive choice for high-stress applications like multi-unit bridges and posterior crowns. Modern zirconia formulations have also significantly improved in translucency.
Understanding the Trade-offs
Selecting a ceramic is a clinical decision based on managing a series of critical trade-offs rooted in the material's composition.
Strength vs. Aesthetics
This is the central compromise in dental ceramics. Increasing the crystalline content (like in zirconia) dramatically increases strength but traditionally reduces translucency, making the restoration more opaque. Conversely, a higher glass content (like in feldspathic porcelain) yields superior, life-like aesthetics but offers lower strength.
Brittleness and Fracture Toughness
While very strong under compression, all ceramics are brittle and can fracture. The crystalline phase, especially in materials like zirconia, acts to stop cracks from propagating. This property, known as fracture toughness, is a measure of the material's resistance to catastrophic failure.
Bondability vs. Cementation
The ability to bond a restoration to the tooth structure is highly dependent on composition. Glassy ceramics can be acid-etched, creating microscopic pits that allow for a strong micromechanical bond with resin cements. Polycrystalline ceramics like zirconia are acid-resistant and cannot be etched in the same way, often relying on specialized primers and traditional cements.
Making the Right Choice for Your Goal
Your clinical objective determines which compositional trade-offs are acceptable and which material is therefore appropriate.
- If your primary focus is ultimate aesthetics for low-stress applications: Choose a predominantly glassy ceramic like feldspathic porcelain for its unmatched translucency.
- If your primary focus is a versatile balance of strength and beauty: Choose a glass-ceramic with high filler content, such as lithium disilicate, for single-unit crowns almost anywhere in the mouth.
- If your primary focus is maximum strength and durability for high-stress areas: Choose a polycrystalline ceramic like zirconia for long-span bridges or crowns on patients with heavy bite forces.
Understanding this relationship between composition and property transforms material selection from a simple choice into a precise clinical decision.
Summary Table:
| Ceramic Type | Primary Composition | Key Properties | Ideal Clinical Use |
|---|---|---|---|
| Predominantly Glassy (e.g., Feldspathic Porcelain) | High glass matrix (silica, feldspar) with some leucite | Superior aesthetics & translucency, lower strength | Anterior veneers, low-stress inlays |
| Glass-Ceramics with Fillers (e.g., Lithium Disilicate) | Balanced glass matrix with high crystalline filler content | Excellent balance of strength & aesthetics | Anterior and posterior single-unit crowns |
| Polycrystalline (e.g., Zirconia) | Almost entirely crystalline (zirconia) with no glass matrix | Maximum strength & fracture toughness, improved translucency | Multi-unit bridges, posterior crowns, high-stress areas |
Ready to select the perfect dental ceramic for your laboratory's needs?
The right material is crucial for the success and durability of every restoration. At KINTEK, we specialize in providing high-quality lab equipment and consumables tailored for dental laboratories. Whether you're working with delicate feldspathic porcelain for veneers or high-strength zirconia for bridges, having reliable equipment ensures consistent, precise results for your clients.
Let us help you achieve excellence in every case. Contact our experts today to discuss your specific requirements and discover how KINTEK can support your laboratory's success.
Visual Guide
Related Products
- Dental Porcelain Zirconia Sintering Ceramic Furnace Chairside with Transformer
- Dental Porcelain Zirconia Sintering Ceramic Vacuum Press Furnace
- Vacuum Dental Porcelain Sintering Furnace
- Hexagonal Boron Nitride HBN Ceramic Ring
- Boron Nitride (BN) Ceramic Plate
People Also Ask
- What is the sintering temperature of dental zirconia? Achieve Maximum Strength & Aesthetics
- What is sintering process in dentistry? Transform Milled 'Chalk' into Durable Dental Restorations
- What is the effect of different sintering process on flexural strength of translucency monolithic zirconia? Optimize Strength vs. Efficiency
- What is the sintering temperature of zirconia ceramic? Mastering the 1400°C-1600°C Thermal Profile
- What is the primary function of a dental sintering furnace? Transform Zirconia into Durable Crowns & Bridges