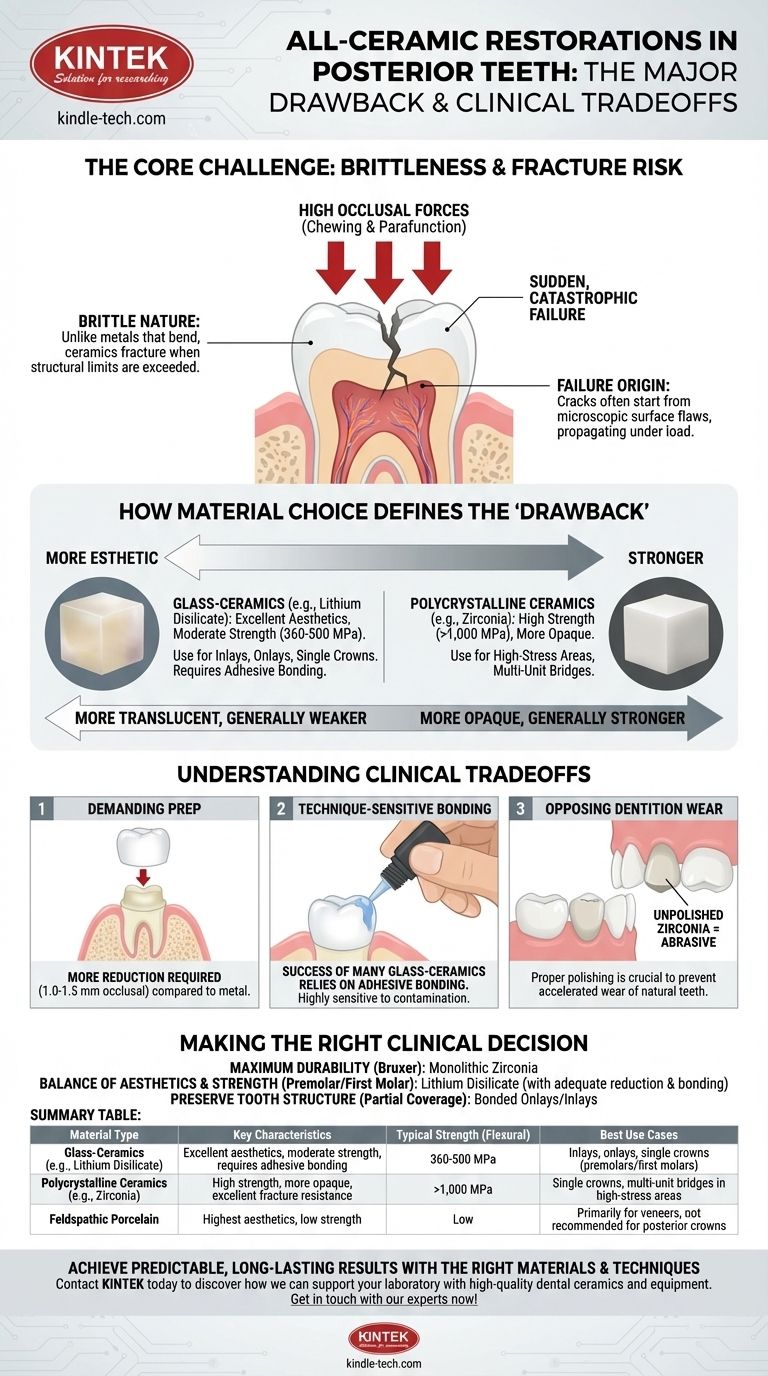
While highly esthetic, the principal drawback of all-ceramic restorations in the posterior mouth is their inherent brittleness and lower fracture toughness compared to metal-based alternatives. This characteristic makes them more susceptible to catastrophic failure under the high occlusal (chewing) forces present in molars and premolars, a risk that is heavily dependent on the specific ceramic material chosen and the precision of the clinical protocol.
The core challenge is not that all ceramics are weak, but that they are unforgiving. Their success hinges on selecting the right material for the specific clinical situation and executing a flawless preparation and bonding technique to mitigate their inherent risk of fracture.

The Core Challenge: Brittleness and Fracture Risk
The posterior of the mouth is a high-demand mechanical environment. All-ceramic materials, while advanced, must be chosen and handled with a deep understanding of their physical limitations to ensure long-term success.
Understanding Material Brittleness
Unlike metals that can bend or deform under stress (ductility), ceramics are brittle. When their structural limit is exceeded, they do not deform; they fracture.
This means a failure is often not a gradual bending but a sudden, catastrophic crack or complete break of the restoration, which can be a significant clinical event.
The Role of Occlusal Forces
Posterior teeth, particularly molars, can exert hundreds of pounds of force per square inch during function and parafunction (like grinding or clenching).
This concentrated, cyclical loading puts immense stress on any restorative material. A brittle material is at a higher risk of crack initiation and propagation under these demanding conditions.
Failure Modes in Posterior Ceramics
Failures often originate from microscopic surface flaws, which can be introduced during manufacturing, chairside adjustments, or even normal wear.
Under occlusal stress, these tiny flaws can propagate, leading to a bulk fracture of the crown or, in the case of bonded restorations, a "chip" or "delamination" of a portion of the ceramic.
How Material Choice Defines the "Drawback"
The term "all-ceramic" encompasses a wide range of materials with vastly different properties. The clinical risk is directly tied to which category of ceramic you use.
Glass-Ceramics (e.g., Lithium Disilicate)
These materials (like Ivoclar's IPS e.max) offer an excellent balance of high esthetics and moderate strength (around 360-500 MPa).
While strong enough for many posterior applications, especially as inlays, onlays, and single crowns, they are not recommended for multi-unit bridges in the molar region. Their success is critically dependent on adhesive bonding and achieving a minimum material thickness.
Polycrystalline Ceramics (e.g., Zirconia)
Zirconia is the strongest ceramic available for dental use, with flexural strengths often exceeding 1,000 MPa. This largely overcomes the classic drawback of fracture.
However, the "drawback" shifts. Traditional zirconia is more opaque, making it less esthetic than glass-ceramics. While newer translucent zirconia options are improving, they often do so at the cost of slightly reduced strength.
The Strength-Aesthetics Spectrum
A fundamental principle exists: the most translucent and life-like ceramics are generally the weakest (e.g., feldspathic porcelain), while the strongest ceramics are the most opaque (e.g., first-generation zirconia). Material selection is always a negotiation along this spectrum.
Understanding the Clinical Trade-offs
Choosing a posterior ceramic involves more than just material science; it has direct clinical implications for your preparation and delivery.
Demanding Tooth Preparation
To compensate for brittleness, ceramics require a specific minimum thickness to resist fracture. This often necessitates more aggressive tooth reduction compared to a full-cast gold crown.
For a posterior zirconia or lithium disilicate crown, you typically need 1.0 to 1.5 mm of occlusal reduction to ensure adequate material bulk and long-term durability. Insufficient reduction is a primary cause of fracture.
Technique-Sensitive Bonding
The success of many glass-ceramic restorations relies on adhesive bonding, not traditional cementation. This process is highly technique-sensitive.
Contamination of the bonding surfaces with saliva, blood, or water can compromise the bond strength, leading to debonding, microleakage, and eventual failure of the restoration.
Wear on Opposing Dentition
While modern, well-polished zirconia has been shown to be kind to opposing enamel, an unpolished or improperly adjusted zirconia surface can be extremely abrasive.
Any chairside adjustments made to a zirconia crown must be followed by a meticulous polishing protocol to restore a smooth surface and prevent accelerated wear of the opposing natural teeth.
Making the Right Clinical Decision
Your material choice should be dictated by a careful analysis of the patient's functional demands, esthetic expectations, and the specific tooth being restored.
- If your primary focus is maximum durability for a bruxer or in a high-stress molar situation: Monolithic zirconia is the most fracture-resistant all-ceramic option, though a full-cast gold crown remains the ultimate standard for longevity.
- If your primary focus is balancing excellent aesthetics and solid strength for a premolar or first molar: Lithium disilicate is often the ideal choice, provided adequate tooth reduction and flawless adhesive bonding can be achieved.
- If your primary focus is preserving tooth structure with a partial coverage restoration: Bonded lithium disilicate onlays and inlays are excellent options that allow for more conservative preparations than a full crown.
Understanding the unique limitations of each ceramic material empowers you to select the right solution for predictable, long-lasting posterior restorations.
Summary Table:
| Material Type | Key Characteristics | Typical Strength (Flexural) | Best Use Cases |
|---|---|---|---|
| Glass-Ceramics (e.g., Lithium Disilicate) | Excellent aesthetics, moderate strength, requires adhesive bonding | 360-500 MPa | Inlays, onlays, single crowns (premolars/first molars) |
| Polycrystalline Ceramics (e.g., Zirconia) | High strength, more opaque, excellent fracture resistance | >1,000 MPa | Single crowns, multi-unit bridges in high-stress areas |
| Feldspathic Porcelain | Highest aesthetics, low strength | Low | Primarily for veneers, not recommended for posterior crowns |
Achieve predictable, long-lasting results with the right ceramic materials and techniques.
At KINTEK, we specialize in providing high-quality dental ceramics and laboratory equipment to support precise, durable restorations. Whether you're working with monolithic zirconia for maximum strength or lithium disilicate for optimal aesthetics, having the right tools and materials is crucial for success.
Let us help you enhance your practice:
- Source reliable materials for consistent, high-strength restorations
- Optimize your lab workflow with equipment designed for precision milling and sintering
- Ensure clinical success by understanding material properties and preparation requirements
Contact us today to discuss your specific needs and discover how KINTEK can support your laboratory in delivering superior all-ceramic restorations. Get in touch with our experts now!
Visual Guide
Related Products
- Silicon Carbide (SIC) Ceramic Sheet Wear-Resistant Engineering Advanced Fine Ceramics
- Vacuum Dental Porcelain Sintering Furnace
- Ceramic Evaporation Boat Set Alumina Crucible for Laboratory Use
- Advanced Engineering Fine Ceramics Alumina Ceramic Saggar for Fine Corundum
- High Quality Alumina Ceramic Screw for Engineering Advanced Fine Ceramics with High Temperature Resistance and Insulation
People Also Ask
- Why is silicon carbide more efficient? Unlock Higher Power Density with SiC's Superior Material Properties
- What are the properties of SiC? Unlock High-Temperature, High-Frequency Performance
- What is the process of making silicon carbide? From Raw Materials to Advanced Ceramics
- What is the type of silicon carbide? A Guide to Polymorphs, Grades, and Applications
- What is the strongest ceramics? Silicon Carbide Leads in Hardness & Thermal Strength